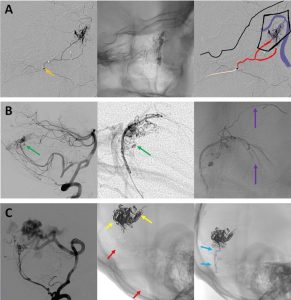
In a case report, Tran et al., from the Department of Neurosurgery, University Medical Center Ho Chi Minh City; the Vascular Department, Cho Ray Hospital, Ho Chi Minh City, Vietnam; and the Department of Neurosurgery, Taichung Veterans General Hospital and National Chung Hsing University, Taichung, Taiwan, published in the American journal of neuroradiology that in selected patients with near-total carotid artery occlusion, where subintimal dissection occurs during endovascular access, the use of a rescue reentry technique with a reentry catheter can be a safe and effective method for achieving successful recanalization and restoring luminal patency 2).
The authors present a single-patient case in which a reentry catheter was used to regain access to the true lumen after unintentional subintimal dissection during an attempt to stent a near-occluded carotid artery. Technical success was achieved, and the patient recovered well.
📉 1. Conceptual Overstatement and Editorial Laxity
This article epitomizes a growing trend in low-yield case reports: elevate the ordinary by inflating the vocabulary. A standard bailout technique, long adapted from peripheral interventions, is glorified as a “rescue reentry technique” as if it were a novel paradigm. This is not a new technique — it’s complication management.
🧩 What they call “rescue,” seasoned neurointerventionists call Tuesday.